Beat four · The case review
A reviewer can see the case and the policy at the same time.
Every criterion links to the packet span that satisfies it and the policy text that requires it. Contradictions, such as left-side pain on one page and right-side pain on another, route to review instead of being silently resolved.
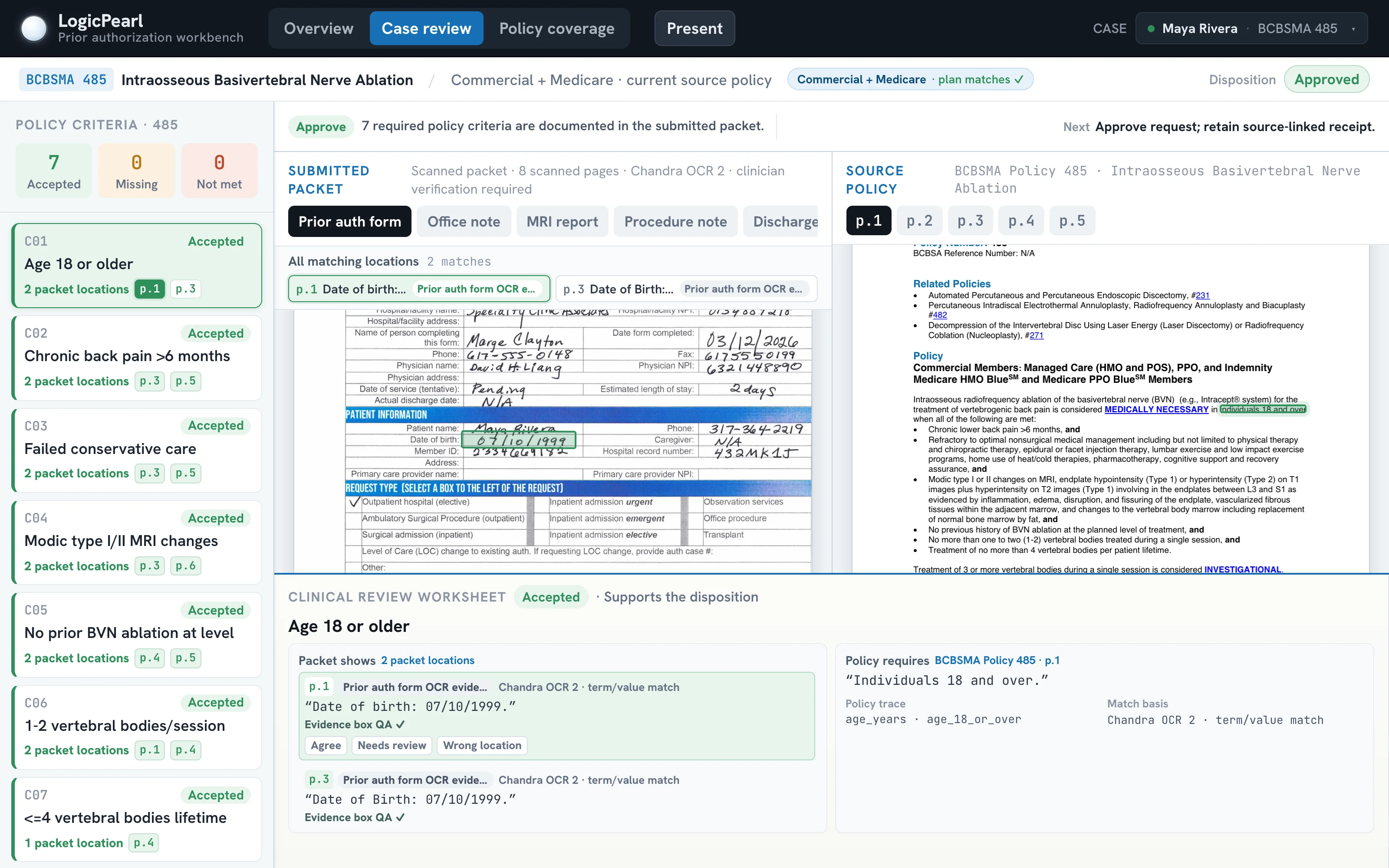
This is the live prior-auth workbench with evidence boxes drawn on the scanned handwriting, criteria linked to packet locations and verbatim policy excerpts, and the audit-ready record behind every disposition. It runs in your browser.